

It is the end of the affair. We are no longer at epidemic levels of covid-19 prevalence in the UK (0.27% of the population infected, where 0.4% is the low end required to be “epidemic”), and all-cause deaths have slipped back below average.

It seems a good time to look back on the extraordinary past few weeks and try and draw conclusions.
First: who has the disease killed? Covid-19 targets the old and the sick; this is not to be callous, but to understand the enemy and to provide context. The average age of those dying of covid-19 in the UK is over 80, and fully a third are residents of care homes where average “stay” (a euphemism I’m afraid) was only 30 months from admission before the virus anyway.
Join Britain’s most civilised publication.

Challenge the consensus. Access rigorous analysis.
Our statistics agencies are only now following Italy’s lead and publishing the comorbidities of those dying from covid-19, and it is now clear just how extreme is the amplification of risk. 95% of victims dying with covid-19 have serious pre-existing conditions: not just background illnesses, but severe enough to be mentioned as causes of death on death certificates. The most prevalent are dementia and diabetes (a quarter of cases, each), hypertension (a fifth) and serious lung, kidney or heart disease (around a sixth each). In both the UK and Italy, the average victim had three comorbidities severe enough to be causes of death on a certificate.
Second: who hasn’t it killed? Parents, unions and nervy adults fret about the risk, but there is little need. With no serious pre-existing conditions, the young-ish and healthy are far more likely to be hit by lightning (49 occurrences per annum in UK) than to die of covid-19 (33 in England under age 40, of which only 3 under the age of 19). Panning out, among healthy under 60s (i.e. children and the vast majority of our working population), 253 people have died of covid-19 in English hospitals; this compares to 400 (non-suicide) drownings per year in the UK. And taking all age-groups where there are no pre-existing conditions serious enough to be mentioned as contributary causes of death, covid-19 has taken about 2/3rds the lives that British roads do every year, and we wouldn’t think of outlawing driving, swimming or going outside in a storm.
Even taking all deaths where covid-19 is mentioned on the death certificate regardless of age or comorbidities, looking at the total toll: 43,000 lives is less than 2018’s excess winter deaths and would count as a bad, but by no means remarkable, influenza year.
Scientific Context
Imperial College haven’t had a good war, and after their performance in other recent epidemics perhaps they will now pass their mantle onto another team. Preferably one that can code to levels fit for publication, never mind policy: it is increasingly awkward to hear the Prime Minister quoting their forecast that, were it not for lockdown, the UK could have been looking at half a million deaths when, at the tail-end of the epidemic, there are only 320,000 deaths worldwide.
But there is more to science than models, and the most accurate analysts were those who relied on other pillars of science than complicated models when input parameters were close to unknown (“garbage in, garbage out”). Science does not only proceed from models after all: it also has, inter alia, experiments, defaults (“null hypotheses”), controls and historical context.
In mid-March, Stanford’s Nobel laureate Michael Levitt (biophysicist and professor of structural biology) discussed the “natural experiment” of the Diamond Princess cruise ship, a virtually perfect sealed petri-dish disproportionately filled with the most susceptible age and health groups. Even here, despite the virus spreading uncontrolled onboard for at least two weeks, infection only reached 20% of passengers and crew (an “upper bound” to infection levels?); Levitt concluded that we must have high levels of innate immunity that can clear the virus. And using very simple mathematics (not “15,000 lines of uncommented code” like Neil Ferguson) he demonstrated that the virus’s spread had never been exponential but rather has been running out of steam from day one. Who listened?
The eccentric biostatistician Knut Wittkowski came at things from a different angle, the “null hypothesis” angle – a default, in layman terms. In the absence of evidence to the contrary, he assumed that covid-19 was a normal viral respiratory disease, and at the end of March wrote a compelling but neglected paper showing how the emerging data backed up his view that “respiratory diseases [including covid-19]… remain only about two months in any given population”.
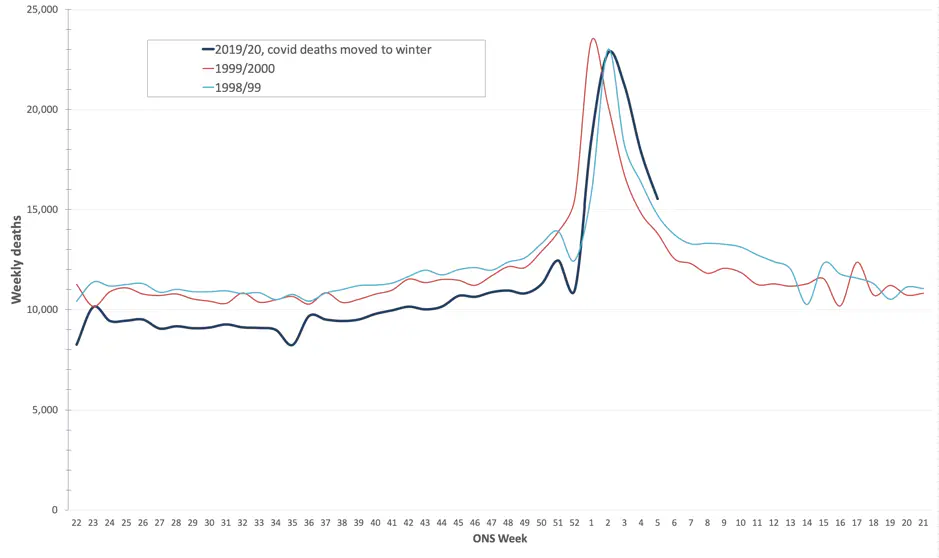
This can be seen in the first graph at the top of this article showing the UK’s epidemic, but is illustrated more clearly by a simple “what-if” thought-experiment: respiratory viral diseases generally peak in mid-winter, and covid-19 is very unusual to be killing people with a peak at Easter. If we simply move covid-19 deaths from spring to winter, the death-toll and the extent of the epidemic is put in the context of recent bad (but not dramatic) influenza years.
Remember the killer flu of 2000, and the lockdown after the Millenium super-spreader events? Me neither. Covid-19 might not be “just flu”, but that’s because there’s no “just” about flu.
We also have ‘controls’, since not all countries have behaved the same. Neither Sweden nor Japan have locked down so, if the lockdown hypothesis were true, Stockholm would by now be a morgue and Greater Tokyo (population 38 million) a necropolis.
In Sweden, Professors Giesecke and Tegnell have managed the epidemic within Sweden’s healthcare capacity without suspending civil liberties or shutting down schools or society (Sir Patrick Vallance’s “Plan A”), with no greater death-toll than our own. The Free Swedes pointed out all along that lockdown would be much easier to get into than out of: no kidding, we’re in an eel-trap.
The final scientific datum would have been historical context. The media has not pointed out that the toll of covid-19 is only 0.5% that of the 1918/1919 influenza, before the advent of antibiotics. Although possible, could Neil Ferguson’s attention-grabbing estimate of twice the number of deaths for covid-19 ever have been realistic when the parameters of the disease were largely unknown? I mean: what were the chances? Oxford’s competing model, trumpeted in the press but attacked by their peers, looks like it will have been far more accurate, so it will be important in due course to ask: why?
Harm done
SAGE minutes make it clear that the public was explicitly petrified in order to ensure compliance with lockdown. Mind-control is objectionable in itself, but has a real cost in lives: before a policy lever like lockdown was pulled, where was the cost/benefit analysis, or was SAGE only thinking of covid-19? Lockdown, after all, affects not just this thing over here (covid-19) but also that thing over there (cancer, cardiac, sepsis, etc.).
Through lockdown, A&E cardiac admissions have been as much as 50% down, so around 5,000 people per month have not been turning up at hospital with heart attack symptoms; heart attacks outside hospital have only a 1-in-10 chance of survival. Same story with strokes. And downstream, many cancers are touch-and-go even if you catch them early; give them a two month head-start and Stanford’s Professor Bhattacharya estimates the impact of urgent cancer referrals running 70% below normal levels will be around 18,000 deaths.
Chris Whitty (CMO) warned two months ago of the toll of these “indirect deaths” (=’lockdown deaths’), and the figures are in: there have been over 13,000 non-covid excess deaths since the start of lockdown, of which over 12,000 in care homes. Can the scale of these figures in the context of the disease be remotely acceptable?
Politics
Where the inevitable enquiry highlights failings, let’s hope they will never be made again. An obvious smoking gun is the government guidance (until 12th March) that it was “very unlikely” that people in care homes will become infected with covid-19. It was already known from the Italian experience that this simply could not be the case given the disease’s target demographic; but as late as mid-April government policy was still for patients to be admitted to care homes from hospitals without requiring negative tests.
Bluntly, this is what South Korea (whose care homes instituted regular temperature checks on all residents with compulsory quarantine for anybody symptomatic, and with two consecutive negative tests required before re-admittance) and Germany (where hospitals are paid for each night a patient is retained, unlike “our” NHS) got right and the UK got lamentably wrong.
Lockdown’s political consequences will be dramatic. What of the impact on the “levelling-up” agenda? The lockdown will prove a peerless inequality wedge: many executives are still busy but a huge number of the lower-waged millions think they’re furloughed but will soon find they’re unemployed. And consider education: it’s increasingly clear that schools should never have closed (so why aren’t they immediately re-opened?), and although private schools have maintained a full curriculum through lockdown, elsewhere many children will have missed out on half a year’s education by September with the damage incalculable.
The damage to the economy is calculable, but dizzying: an extra £300 to 500 billion deficit (let me help you: 10 to 15 Brexit bills, with lockdown now costing a Brexit bill per week) will mean higher taxes, higher borrowing and therefore (the other side of the equation) less investment. Geographically, investment will refocus where it always made sense, not in the locations where, politically, it is most needed. If the lockdown tanker isn’t turned around soon, the “northern powerhouse” agenda will wither on the vine and the mortar is already falling out of the Red Wall. (Sorry for the mixed metaphors but you get the point.)
Next time
Kids can’t make it through a day at school without having “growth mindset” hammered into them, so let’s acknowledge failings and learn lessons from this shambles, and make sure that the next epidemic meets defences ready to resist it:
- The Nightingales: is there a case to have spare hospitals mothballed and dust-sheeted, ready at a moment’s notice for the inevitable next time, rather than having to put the rest of the NHS into hibernation during an epidemic at such cost to life? Of course, this is no good without the staff, so:
- Remember the 750,000-strong ‘NHS volunteer army’: would basic annual training (like a medical Territorial Army) allow us to hit future epidemics with phalanxes of trained staff ready to go?
- Given the high incidence of asymptomatic spread, contact-tracing can’t work with this virus notwithstanding the horlicks made of setting up the NHSX app. But perhaps the next killer, the “disease X”, will be amenable to such an approach, and we should have the app and other tracing measures ready to go at a moment’s notice.
- PPE: how on earth could we run out so early in an epidemic? And treatment protocols changed during the epidemic such that the ventilators weren’t needed; but maybe they will be next time.
Let’s not be caught on the hop again.
For now: we’re bamboozled with daily changes to the semi-mystical R number (cognoscenti have moved onto Z-scores), but dig below the surface and it’s clear that transmission is now mostly within care homes and hospitals (up to 20% of infections are now nosocomial), and even there it is in rapid retreat. So why on earth is civil society still locked down?
Boris Johnson’s hero was not famous for “grandmother steps”, and it is clearer every day that (despite the polls) the lockdown is causing more harm than good; Churchill would grit his teeth, rip the plaster off, and get the country back to school and back to work.


